
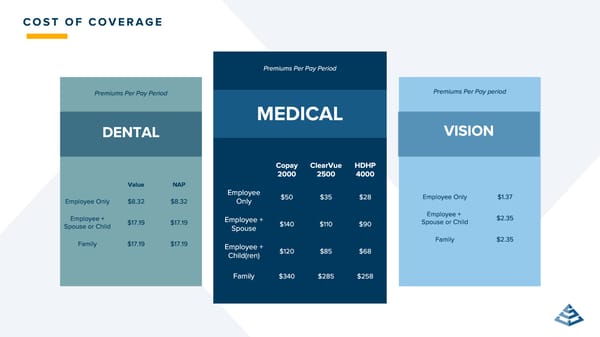
C O S T O F C O V E R A G E DENTAL Premiums Per Pay period VISION Premiums Per Pay Period MEDICAL Premiums Per Pay Period Copay 2000 ClearVue 2500 HDHP 4000 Employee Only $ 50 $ 35 $ 28 Employee + Spouse $ 140 $ 110 $ 90 Employee + Child ( ren ) $ 120 $ 85 $ 68 Family $ 340 $ 285 $ 258 Value NAP Employee Only $ 8 . 32 $ 8 . 32 Employee + Spouse or Child $ 17 . 19 $ 17 . 19 Family $ 17 . 19 $ 17 . 19 Employee Only $ 1 . 37 Employee + Spouse or Child $ 2 . 35 Family $ 2 . 35
 ClearVue Glass & Mirror Company Benefits Guide 2026 Page 26 Page 28
ClearVue Glass & Mirror Company Benefits Guide 2026 Page 26 Page 28