
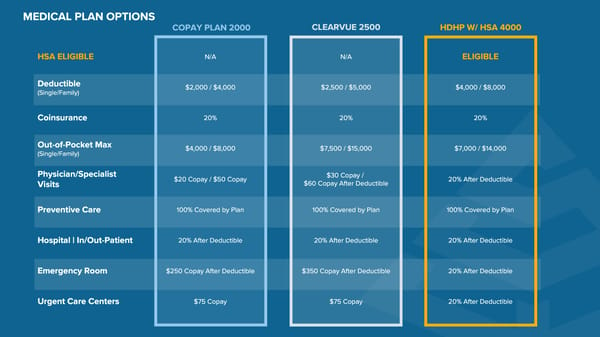
HDHP W / HSA 4000 CLEARVUE 2500 HSA ELIGIBLE N / A N / A ELIGIBLE Deductible ( Single / Family ) $ 2 , 000 / $ 4 , 000 $ 2 , 500 / $ 5 , 000 $ 4 , 000 / $ 8 , 000 Coinsurance 20 % 20 % 20 % Out - of - Pocket Max ( Single / Family ) $ 4 , 000 / $ 8 , 000 $ 7 , 500 / $ 15 , 000 $ 7 , 000 / $ 14 , 000 Physician / Specialist Visits $ 20 Copay / $ 50 Copay $ 30 Copay / $ 60 Copay After Deductible 20 % After Deductible Preventive Care 100 % Covered by Plan 100 % Covered by Plan 100 % Covered by Plan Hospital | In / Out - Patient 20 % After Deductible 20 % After Deductible 20 % After Deductible Emergency Room $ 250 Copay After Deductible $ 350 Copay After Deductible 20 % After Deductible Urgent Care Centers $ 75 Copay $ 75 Copay 20 % After Deductible MEDICAL PLAN OPTIONS COPAY PLAN 2000
 ClearVue Glass & Mirror Company Benefits Guide 2026 Page 7 Page 9
ClearVue Glass & Mirror Company Benefits Guide 2026 Page 7 Page 9