
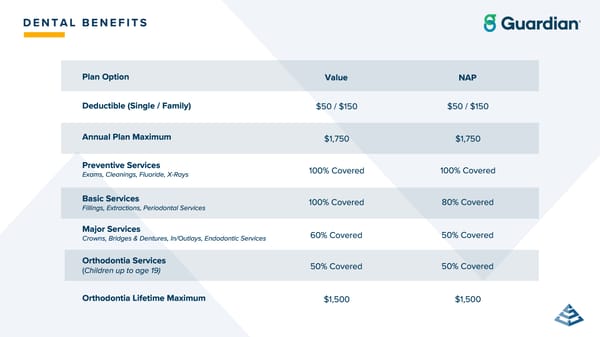
Annual Plan Maximum $ 1 , 750 100 % Covered 100 % Covered 60 % Covered 50 % Covered Deductible ( Single / Family ) $ 50 / $ 150 $ 1 , 500 Orthodontia Lifetime Maximum Preventive Services Exams , Cleanings , Fluoride , X - Rays Basic Services Fillings , Extractions , Periodontal Services Major Services Crowns , Bridges & Dentures , In / Outlays , Endodontic Services Orthodontia Services ( Children up to age 19 ) D E N T A L B E N E F I T S $ 1 , 750 100 % Covered 80 % Covered 50 % Covered 50 % Covered $ 50 / $ 150 $ 1 , 500 Plan Option Value NAP
 ClearVue Glass & Mirror Company Benefits Guide 2026 Page 23 Page 25
ClearVue Glass & Mirror Company Benefits Guide 2026 Page 23 Page 25